

Obesity / Type 2 Diabetes
Morbid obesity is now recognized by the entire scientific community as a disease that poses serious risks to the health and lives of patients evolving to a global epidemic.
Conservative treatment, which includes changes in eating habits and taking special medications, is often not enough to solve the problem of obesity and many times the benefits are temporary.
The most effective approach in the treatment of morbid obesity is the so-called Metabolic Surgery.
The term reflects the modern treatment of the disease, offering hope not only for significant and lasting weight loss (Bariatric Surgery) but also for the parallel treatment of all conditions that occur as a result of obesity, such as type 2 diabetes, hypertension and coronary heart disease.
Dr. Konstantinidis and his Surgical Team have extensive experience in performing the full range of Metabolic Surgery or Obesity Surgery, using the robotic system da Vinci Xi, at Athens Medical Center.
This is the most modern approach to Metabolic Surgery that ensures the best medical outcome with optimal aesthetics and minimal complications.
From the first moment, Dr. Konstantinidis and his Surgical Team will be close to you to help you set the right goals for your health and choose the type of surgery that suits your desires and priorities.
For this purpose, Dr. Konstantinidis and his Surgical Team apply a holistic approach for each patient individually, having close collaboration with leading scientists from various medical specialties of Athens Medical Group related to the treatment of morbid obesity and its complications, such as cardiologists, pulmonologists, gastroenterologists, radiologists, dieticians and psychologists.

What is Disease Obesity?
In order to be able to objectively define obesity and its severity, we use various indicators, with the simplest being the Body Mass Index (BMI).
Obesity is defined as pathogenic when BMI is greater than or equal to 40 or greater than or equal to 35 in the presence of concomitant diseases resulting from obesity.
It is worth noting that the survival rate of morbidly obese people is 20 years lower than non-obese people of similar age.
Patients with a BMI> 50 are classified as obese. A more aggressive therapeutic approach is required for these patients.
Why choose Dr. Konstantinidis?
Dr. K. M. Konstantinidis and his team possess vast experience in the field of laparoscopic and robotic surgery.
Dr. Konstantinidis is the pioneer of Robotic Surgery in Greece and one of the leading figures internationally in the field, having performed the largest series of General Surgery operations in Europe with the innovative Da Vinci® robotic system, including inguinal hernia surgeries.
How common is Obesity?
According to recent research worldwide, obesity is considered the second most preventable pathogenic cause of death after smoking.
Indicative of its high risk is that it causes three times more deaths than bowel and breast cancer combined!
Suffice it to say that more than 1/6 of the world’s population are overweight.
Of these, at least 300,000,000 suffer from morbid obesity.
In Greece, scientists are ringing the alarm bell to the increase of obesity levels in the general population.
According to the European Statistical Office (Eurostat), Greece ranks first within Europe in obesity with 26.7% while it shares second place along with the United Kingdom (prior to Brexit) in women’s obesity with 17.8%.
What causes morbid Obesity?
The pathogenesis of morbid obesity is quite complex.
The most important predisposing factor for obesity is heredity (20-30%). When one of the parents is obese, the theoretical probability of obesity for the children is 40%, whereas if both parents are obese, the probability is doubled (80%)!
Although a small number of people appear to be genetically protected from obesity, the vast majority of people are vulnerable.
Also, “benign” hypertension in childhood negatively affects the metabolic rate, increases the number of fat cells and predisposes to obesity in adulthood.
The influence of various social, educational, economic and psychological factors is also important. Lack of information, sedentary lifestyle and unhealthy diet can easily lead to obesity, as well as certain psychogenic factors such as anxiety and stress.
In rare cases, obesity may be due to some hereditary metabolic disorders (e.g. Prader Willi syndrome, Cohen syndrome, etc.).
Essentially, the phenomenon of obesity is largely due to modern lifestyle and its characteristics, such as the abundance of food high in sugar, fat and calories, as well as sedentary work and lack of physical activity.
What are the complications of Obesity?
Obesity is a disease associated with a number of concomitant health problems and dangerous diseases, such as:
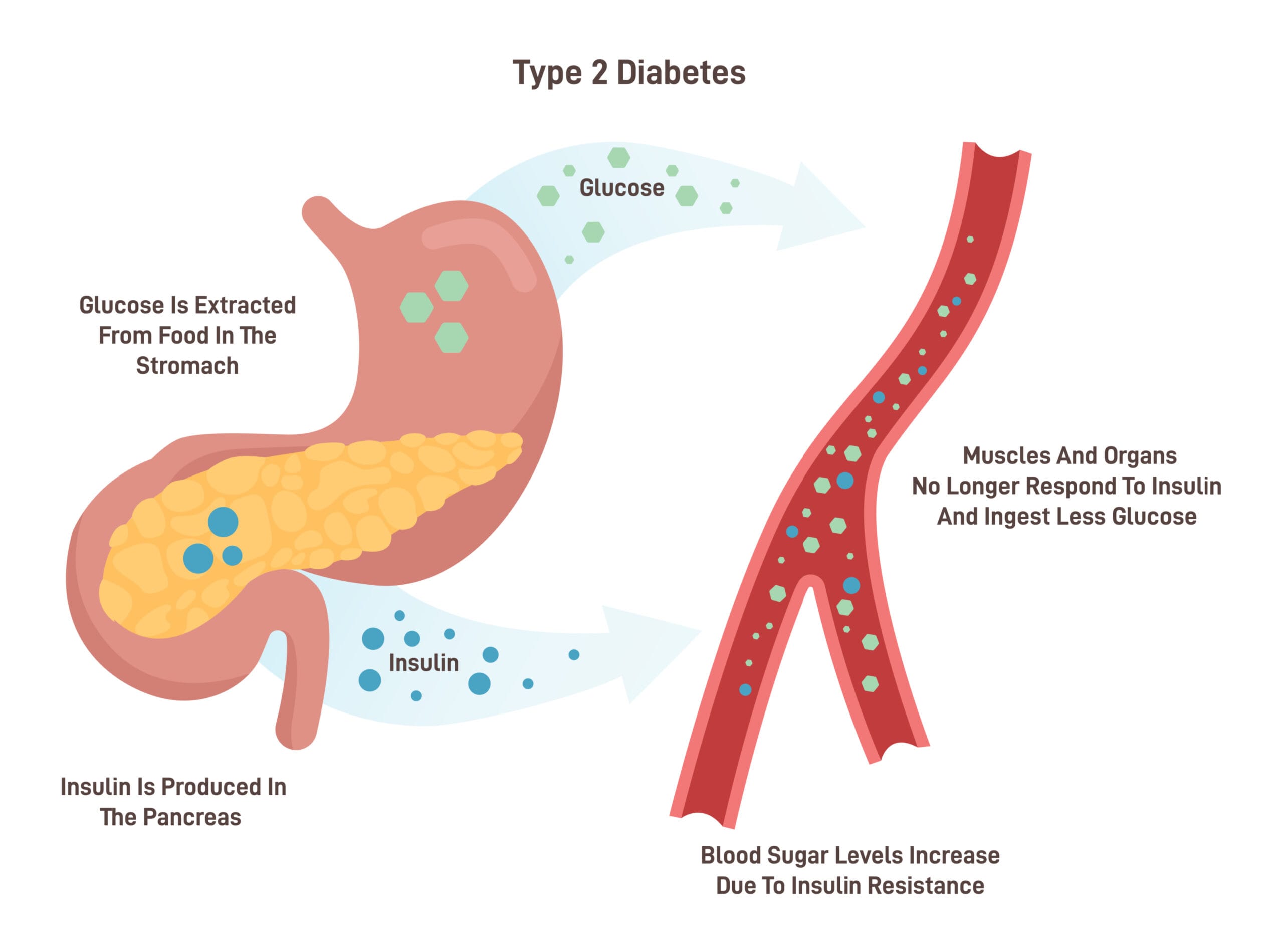
- Endocrine / Metabolic: Insulin Resistance, Diabetes, Dyslipidemia, Menstrual Disorders, Inability to Have Children
- Cardiovascular: Hypertension, Coronary heart disease, Arrhythmias, Pulmonary hypertension, Heart failure, Stroke, Venous insufficiency, Varicose veins, Venous thrombosis, Pulmonary embolism
- Pulmonary: Abnormal spirometry tests, Sleep Apnea, Hypoventilation Syndrome
- Musculoskeletal: Back pain, Osteoarthritis of the lower extremities, Gout
- Gastrointestinal: Gastroesophageal Reflux, Gallstones, Pancreatitis, Fatty Liver Filtration, Non-alcoholic Steatohepatitis
- Cancers: Colon, Prostate, Breast, Uterus, Gallbladder
- Others: Headache, Hernias, Urinary Incontinence in Effort, Psychological Disorders
How is Obesity treated?
Metabolic Surgery is the only treatment that can maintain long-term weight loss and therefore deal safely and effectively with both morbid obesity and the serious health problems that accompany it, such as type 2 diabetes.
More and more obese patients are being treated surgically because the growing experience of specialized surgery centers leads to more permanent results and therefore a reduction in morbidity and mortality.
Now, Metabolic Surgery is performed with Minimally Invasive Methods, such as Laparoscopy, which have an advantage over the respective open procedures in ensuring shorter hospital stay, the least incidence of respiratory complications, the minimization of the injury rates as well as speedier return on activity and work postoperatively.
An evolution of laparoscopy is Robotic Surgery, which maximizes advantages of the former and eliminates any of its shortcomings, offering incomparable stability, flexibility and precision in surgical movements, as well as access to even the most inaccessible areas.
This ensures the least possible tissue injury during surgery.
There are four types of surgery, performed almost exclusively with laparoscopy:
- Restrictive: gastric ring, sleeve gastrectomy
- Malabsorbing: enterectomy, duodenal bypass switch
- Mixed type procedures: gastric bypass, biliopancreatic diversion (bypass)
- Procedures that modify gastric motility: gastric pacemaker
What type of surgery should I choose?
Dr. Konstantinidis and his Surgical Team perform the full range of Metabolic Surgery, with the assistance of the state-of-the-art robotic system da Vinci Xi, at Athens Medical Center, Maroussi.
From the first moment, each patient is treated as a unique, special case.
Dr. Konstantinidis and his associates suggest the type of surgery that is suitable for each patient based on his/her state of health, as well as the goals set.
At the first meeting the patient is informed in detail and all the necessary information is provided. At the same time, the surgeon receives a complete medical history.
In the next steps, the patient is examined and his/her condition is evaluated by a team of doctors of various specialties, such as cardiologists, gastroenterologists, etc., in order to ensure the best possible outcome from the surgery.
Who are ideal candidates for Metabolic Surgery?
In order for an obese person to end up in the operating room, specific, reliable and acceptable criteria, supported by the international literature, must be met, such as:
- BMI> or = 40 or BMI> or = 35 with severe obesity-related conditions
- Repeated unsuccessful attempts of the obese person to lose weight with conservative methods (diet) for at least two years
- Good information and understanding by the patient about the possibilities, limitations and complications of the procedure
- Absence of alcoholism, psychosis or uncontrolled depression
- Acceptable surgical risk
Gastric Sleeve
Sleeve robotic gastrectomy
What is Robotic Sleeve Gastrectomy?
Sleeve gastrectomy is a method that is finally gaining ground because it is performed relatively simply, laparoscopically, and ideally with robotic surgery.
It is a restrictive operation, where the patient loses weight due to the reduction of food that can be consumed.
Robotic sleeve gastrectomy aims to shrink the patient’s stomach. This is accomplished after removing part of the organ, after which the stomach looks like a sleeve.
As a result, the size of the stomach is reduced without affecting its functions (e.g. vitamins are normally received from food and there is no need for vitamin supplements).
In addition, the part of the stomach that is removed produces an appetizing hormone that is responsible for creating the feeling of hunger (ghrelin).
Therefore, after the operation the patient does not feel the same need to consume food allowing for the weight to gradually decrease and stabilize at low levels.
What are the advantages of Robotic Sleeve Gastrectomy?
Robotic sleeve gastrectomy offers great benefits to the patient, with the biggest being the significant reduction of the risk of complications than in non-robotic procedures.
In particular, with the help of the state-of-the-art robotic system, da Vinci Xi:
- no foreign bodies remain (e.g. mesh, ring) and the incisions are small so there is less chance of postoperative complications
- robotic precision in surgical movements significantly reduces the risk of leakage into the gastric fundus, often a serious complication that may require reoperation to treat
- the risk of injury to arteries and nearby organs, such as the spleen, which can lead to splenectomy, is avoided
- the operation is bloodless
- postoperative pain is minimal
- the stay of the patient in the hospital is shorter
- recovery is faster
- better control of movements by the surgeon can reduce the cost of consumables for the operation
- an excellent cosmetic outcome is achieved – As a whole, the operations performed with the robotic system da Vinci Xi, are all carried out in a straight line, exuding symmetry
- special emphasis is always placed on the convergence of wounds anatomically in layers, in order to minimize the risk of complications, such as postoperative hernias
Also, the use of the robot offers significant advantages to the surgeon:
- the robotic arms eliminate the natural tremor of the hand and perform the surgical movements with absolute precision and stability.
- robotic arms have great flexibility so they can access even places beyond human reach
- the surgeon avoids extreme physical fatigue, as he is seated in front of a special console that allows him to navigate the robotic arms, through a large 3D screen
- the ability to 3D viewing and digitally magnify the surgical field creates the feeling that the surgeon’s hands are inside the patient’s body
Gastric Bypass
Robotic Gastric Bypass
What is Robotic Gastric Bypass?
Gastric bypass is currently the most commonly used type of metabolic surgery, due to its particularly good results in weight loss.
At ten-year follow-up, most patients maintain a loss of at least 50% of excess weight.
It is the most commonly performed type of bariatric surgery (accounting for 65% of bariatric procedure worldwide) and is usually performed with conventional laparoscopy or ideally with robotic surgery.
The great advantage of the method is that it can be applied to patients who consume a lot of sweets and also to over-obese patients, since the weight loss is greater than after restrictive surgery.
During gastric bypass, a small “pouch” is created in the upper part of the stomach and in addition a small diversion of the intestine is made, in order to reduce the length of the small intestine to 5 meters.
The average duration of the procedure ranges from 2 to 4 hours and the average hospital stay is 4 to 5 days.
This method leads to a loss of 65-85% of excess weight and improvement or complete remission of concomitant diseases, such as hypertension, type 2 diabetes and sleep apnea syndrome.
Complications, although rare, include gastrointestinal stenosis, internal hernias, anastomotic ulcer, and leakage from the suture line.
Gastric Ring Removal - Gastric Obstruction Repair
Laparoscopic Gastric Banding
What is Laparoscopic Gastric Banding?
One of the most common methods of surgical treatment of morbid obesity is the placement of a gastric band, laparoscopically.
During the operation, an adjustable silicone band in the form of a ring is placed around the upper part of the stomach, dividing it into two parts.
The small bag in the upper part of the stomach can only hold a small amount of food, thus reducing the amount and calories consumed.
The diameter of this band determines the rate at which food leaves the new stomach pouch and is regulated by a special subcutaneous valve.
The ring used by Dr. Konstantinidis is the only one approved by the US Food and Drug Administration (FDA).
Adjustments to the gastric band should be made according to the degree of weight loss of a patient over time. The indications for adjustments, as well as the right time at which they should be made, concern physical, nutritional and psychological factors.
What are the benefits of Laparoscopic Gastric Banding?
Laparoscopic gastric banding is the least traumatic method of treating obesity and is accompanied by many important advantages:
- The operation is performed laparoscopically and no incisions, sutures or other related procedures are required during the placement of the band.
- The size of the small part of the stomach, as well as the diameter of the opening between its two parts can be precisely decided, while no additional intervention is required to adjust the diameter of the opening.
- It does not cause irreversible damage. The ring can be removed without problems, although, of course, this is not the purpose of its placement.
- The average duration of the procedure ranges from 30 to 90 minutes and the patient usually returns home within 24 hours after the laparoscopic operation.
- 60% to 80% of the extra weight is lost within 12 to 18 months.
- After the operation, a large percentage of reversal of the health problems caused by obesity is achieved.
How is the Gastric Band properly adjusted?
Adjustments to the gastric band should be made according to the degree of weight loss of a patient over time. The indications for adjustments, as well as the right time at which they should be made, concern physical, nutritional and psychological factors.
According to the literature, the adjustments are made according to the patient’s feeling of satiety.
The sense of satiety may stem from biological factors, but also psychological.
In the case of biological satiety, usually caused by a large reduction in body weight (e.g. 10 to 15kg), there is absolute indication for adjustment, as the band must be adjusted to a smaller stomach, as a result of weight loss.
In the case of psychological satiety, however, the patient may have satisfied the feeling of biological hunger but may want to consume more food for emotional reasons.
Therefore, regulation in this context may prove ineffective, as the ring puts more pressure on the stomach than is necessary for the passage of food, resulting in the possibility of serious long-term complications (e.g. band slippage, gastric pouch dilatation, stomach erosion, etc.).
The biological feeling of hunger and the appetite that a person may have are two different things that are connected. There is a quite common confusion between “I am hungry” and “I want to eat” because the two processes share the same brain center and have common biochemical mechanisms.
It is important to fully evaluate the causes of the feeling of hunger and satiety accordingly, in order to proceed to a new regulation.
In this process undertaken by the team of specialists who monitor each of our patients, for the decision of the right time of an arrangement, the patient actively participates.
In this context the patient is offered a special training to learn to recognize the biological signs of hunger and to differentiate them from emotional signals, such as “I’m tired of eating a little sweet to stimulate me”, or environmental, such as ” I saw a sweet and I wanted it “.
Education and scientific principles for proper regulation help the patient to take advantage of the regulation properly resulting in weight change and eating behavior.
What are the principles of proper regulation?
A proper gastric band adjustment is subject to the following principles:
- The level of adjustment (i.e. the amount of fluid flowing into the band through the valve) should be sufficient to achieve a prolonged satiety sensation in the patient.
- Weight loss should be steady and progressive, with a loss of approximately 0.5 to 1kg of adipose tissue / week.
- No regulation should cause restraint symptoms (e.g. vomiting, heartburn, excessive difficulty in consuming a normal amount of food).
- Achieving the ideal body weight should be planned with a realistic goal ranging from 12 to 18 months after surgery, although in the case of extremely morbid obesity (BMI> 50) more time may be required.
In our patients, the adjustments are always made after clear indications, according to their medical, nutritional and psychological profile, and after the consent of the surgeon and his scientific team.
Thus, the problems are minimized and the patient has a proper weight loss, without complications.
Laparoscopic gastrectomy and biliopancreatic bypass with duodenal diversion
What is Laparoscopic gastrectomy and biliopancreatic bypass with duodenal diversion?
In this procedure, a peripheral gastrectomy is performed, i.e. a large part of the stomach is removed. The small intestine is dissected in its last part and anastomosed to the remaining stomach. Only a small part of the small intestine remains, in which the food meets the biliopancreatic fluids to start its absorption.
Research on biliopancreatic bypass (Scopinaro) showed 83% complete control of diabetes and 17% improvement.
As a first mechanism of action, in biliopancreatic bypass, small absorption of fat from the diet is caused, leading to intramuscular fat consumption.
Thus, the body returns to the use of glucose as an energy source with the consequent disappearance of insulin resistance.
The second and third mechanism of action are the diversion of the duodenum and the stimulation of the final ileum by contact with food.
Incretins are intestinal hormones that have the ability to stimulate insulin secretion by the β-cell. They are mainly represented by the GIP secreted in the duodenum and the GLP-I secreted in the final ileum.
The short bowel hypothesis is based on this very bypass of the duodenum, which is thought to be responsible for the pathophysiology of type 2 diabetes.
An excessive reaction of the duodenum to food stimulation causes hypersecretion of incretins and therefore insulin. Insulin resistance represents the body’s defense mechanism to this phenomenon.
In response to this theory, Rubino formulated the theory of anti-incretins. He suggested research into unknown “anti-incretins”, which are produced by a pathological duodenum when stimulated by food and interact with the action of normal incretins. In both cases the duodenum bypass solves the problem.
According to the theory of the distal intestine, the beneficial effect of both biliopancreatic and gastric bypass is due to the release of strong incretins from the mucosa of the ileum and specifically GLP-I which:
- improves β-cell function,
- stimulates β-cell proliferation and
- reduces β-cell apoptosis
Gastric bypass Roux-en-Y
What is a Gastric bypass Roux-en-Y?
A large portion of the stomach is isolated with staples to create a smaller pouch to retain food.
The small intestine is then dissected at the beginning of the jejunum and anastomosed to the gastric cavity that has formed. This shortens the digestive tract and reduces the absorption of some substances (malabsorption).
What should be the attitude of the patient after surgery?
Patients have already made a serious decision to deal with the problem of morbid obesity, so they should strictly follow the doctor’s instructions.
It is important to follow the meal plan and all other instructions.
In addition, patients should avoid sweets and alcohol, start walking, exercising and staying active for life.
Obesity surgery today offers a safe, successful and permanent treatment for people with morbid obesity.
When all other methods have failed, it is necessary to discuss with a surgeon specialized in laparoscopic surgery.
This solution paves the way for a normal life again!
Gastric Band removal
Problems that sometimes arise from the placement of a gastric band with the aim of losing weight, can lead to the need for its removal.
In some cases, removal of the gastric band may be reconsidered in another surgical procedure to maintain and improve long-term weight loss and avoid the health problems associated with obesity.
Regardless of the way in which the gastric banding surgery was performed, the procedure of choice for its removal is laparoscopy or for an even higher level of safety and efficiency, robotic surgery.
The minimally invasive nature of the surgery allows patients to be discharged even on the same day or to remain in the hospital for one to two more days, depending on whether there is a parallel medical condition that requires care.
When is it appropriate to remove the Gastric Band?
The removal of the gastric band is indicated for the following cases:
- lack of adequate weight loss
- band corrosion
- band infection
- symptoms of band intolerance (nausea, vomiting or persistent discomfort or pain)
- band slippage
- difficulty swallowing
- esophageal dyskinesia
- gastroesophageal reflux
- infection of the band gate
- inversion or relocation of the band door
Gastric folding resolution
Gastric folding is a laparoscopic procedure in which the stomach is folded and sutured.
As a result, the capacity of the stomach shrinks, creating the feeling of fullness with a much smaller amount of food.
If, however, the result of weight loss surgery is not the desired one or there are complications related to the folding of the stomach, then the gastric folding can be resolved and possibly revised into another surgical procedure to treat obesity.