

Rectal Prolapse
Prolapse of the rectum is a condition that directly affects the patients’ lifestyle, degrading their daily life and limiting their independence.
International pioneers in robotic surgery, Dr. Konstantinidis and his Surgical Team focus on improving the overall health and quality of life of those suffering from rectal prolapse, using the most modern treatments, such as robotic rectopexy, with exceptional success and lower complication rates.

What is Rectal Prolapse?
Prolapse of the rectum occurs when the rectum, i.e. the last part of the large intestine, falls from within the pelvic area and down to the anus. At an advanced stage of prolapse, the rectum may stick out through the anus.
As a condition it is relatively rare, especially in children. It occurs more often in adults over the age of 50 and more in women than in men. About 80% – 90% of cases of rectal prolapse involve women.
Why choose Dr. Konstantinidis?
Dr. K. M. Konstantinidis and his team possess vast experience in the field of laparoscopic and robotic surgery.
Dr. Konstantinidis is the pioneer of Robotic Surgery in Greece and one of the leading figures internationally in the field, having performed the largest series of General Surgery operations in Europe with the innovative Da Vinci® robotic system, including inguinal hernia surgeries.
What are the symptoms of Rectal Prolapse?

Symptoms of rectal prolapse include:
part of the rectum sticks out through the anus, in the form of a reddish mass
constipation or diarrhea or both
feeling of incomplete emptying
bleeding
fecal incontinence
Without treatment, symptoms such as constipation and bowel control problems (fecal incontinence) can deteriorate.
Over time, the rectum may slip and stick out through the anus more often and more easily.
In case of heavy bleeding or prolapse of the rectum that cannot be pushed back into the body, patients should seek immediate medical attention.
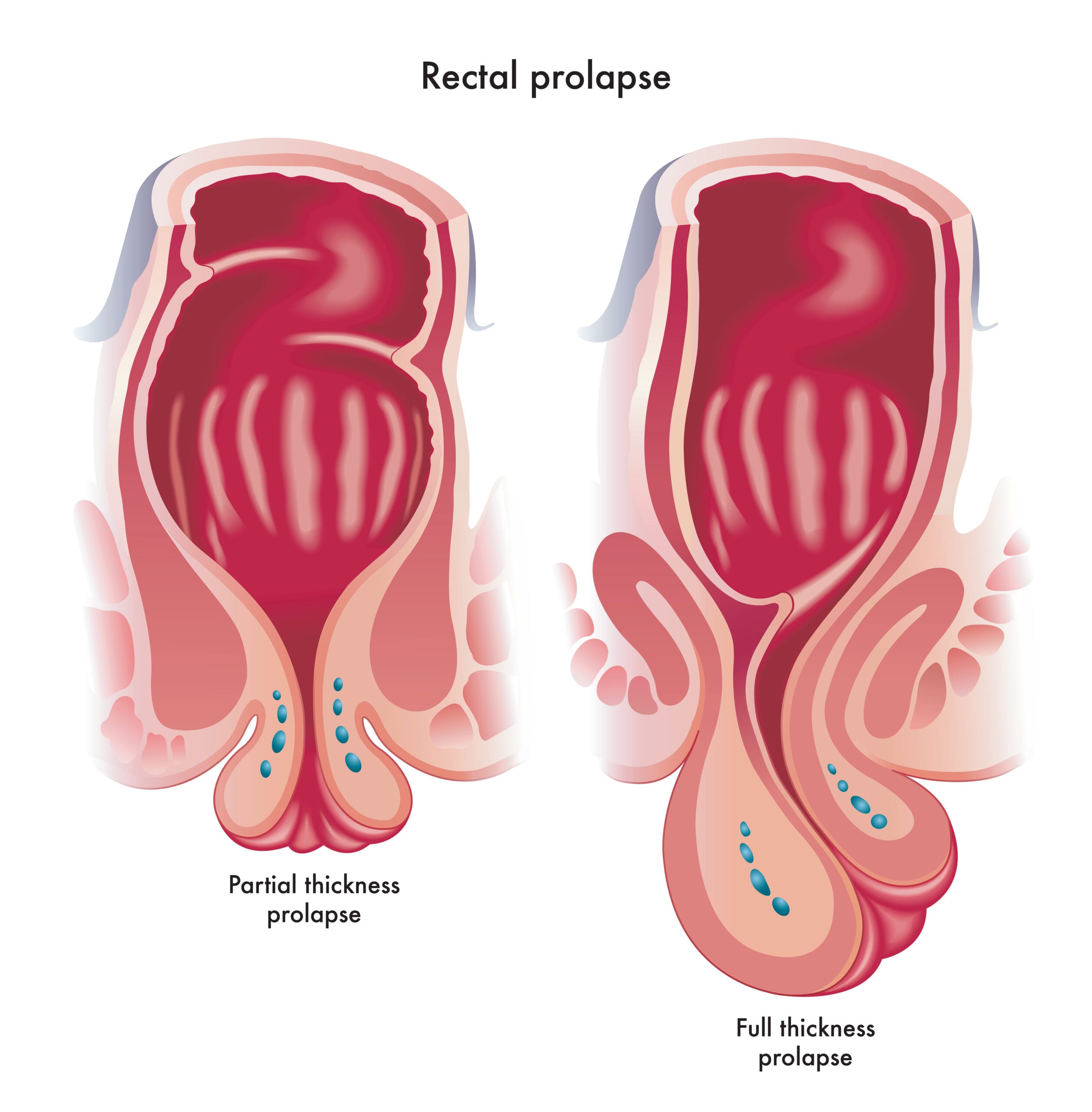
How many types of Rectal Prolapse are there?
There are three types of rectal prolapse:
- Partial prolapse (otherwise known as mucosal prolapse): The mucous membrane of the rectum slips and usually sticks out through the anus.
- Total prolapse: The entire wall of the rectum slips and usually sticks out through the anus. In the beginning, this only happens during bowel movements. As the disease deteriorates, the rectum may stick out permanently.
- Internal prolapse: A part of the rectal wall slides within or over another part. In this case the rectum does not protrude from the anus.
What causes Rectal Prolapse?
Chronic constipation occurs in 30-67% of cases of rectal prolapse, while an additional 15% of patients experience chronic diarrhea.
In the past, the development of rectal prolapse was associated with multiple normal births. However, a large percentage of women with rectal prolapse have never had children.
Some women with rectal prolapse have weak pelvic floor muscles and may also have other related health problems, such as:
- intestinal hernia, i.e. hernia in the small intestine
- rectοcele, i.e. a herniation of the front wall of the rectum into the back wall of the vagina
- vesical hernia, i.e. swelling or prolapse of the bladder into the vagina
- prolapse of the uterus or vagina
What are the risk factors for Rectal Prolapse?
Prolapse of the rectum has been associated with the following risk factors:
- cystic fibrosis
- intestinal infections due to certain parasites
- previous pelvic floor surgery
- intense cough
What are the complications of Rectal Prolapse?
If left untreated, rectal prolapse can result in the following complications:
- ulcers in the rectum, which can cause bleeding
- damage to the muscles and nerves of the sphincter, causing or worsening fecal incontinence
It should be noted that when the prolapsed rectum cannot be pushed back into the body, this constitutes an emergency medical condition, as the blood supply to that part of the rectum may be interrupted.
How is Rectal Prolapse diagnosed?
The diagnosis of rectal prolapse begins with obtaining a medical history and clinical examination.
At the same time, depending on the case, some of the following examinations may be performed:
- proctoscopy / orthoscopy
- colonoscopy
- rectal manometry
- stool chart
- barium meal
- magnetic resonance proctography
How is Rectal Prolapse treated?
Treatment of rectal prolapse depends on the age and general health of the patient, as well as the type and severity of the condition.
If prolapse is at an early stage, then appropriate treatment may be conservative and include a high-fiber diet to treat constipation that may contribute to prolapse, and pelvic floor physiotherapy (Kegel exercises).
In more advanced stages of the condition, however, the treatment is surgical and it involves the following procedures, depending on the case:
- Resection of rectal mucosa (Delorme Surgery): It is common in cases of partial prolapse and it involves the resection of the mucosa in the part of the rectum that falls. The rectal muscles are then folded and sutured.
- Perineal rectosigmoidectomy (Altemeier surgery): Performed through the anus, without abdominal incision. During the operation, the rectum is deliberately pulled out of the body and then the excess is excised and the rest of the rectum is reconnected with the anus.
- Rectopexy: The rectum is prepared, pulled up and fixed to the pelvis with or without the use of a mesh. This is a method with high success rates. Rectopexy can be performed with open surgery or with a minimally invasive technique, i.e. laparoscopy or robotic surgery.
Perineal rectosigmoidectomy and resection of the rectal mucosa are operations that do not involve incisions and are performed through the anus.
In contrast, rectopexy is an intra-abdominal procedure involving a large incision (conventional open surgery) or small holes (laparoscopic – robotic rectopexy).
Rectopexy has a lower recurrence rate than other treatments.
ROBOTIC RECTOPEXY
What is Robotic Rectopexy?
Robotic rectopexy is the evolution of the equivalent laparoscopic procedure, involving the use of a state-of-the-art robotic system (in this case the da Vinci Xi system, at Athens Medical Center).
Like laparoscopy, robotic rectopexy is a minimally invasive procedure that involves opening small holes, a few millimeters long, through which the surgeon can insert a camera and special surgical instruments into the patient’s abdomen.
Robotic tools are smaller than the laparoscopic ones and as a result, the holes that are opened during robotic orthopedics are slightly smaller.
In addition, the surgeon enjoys 3D imaging of the surgical field with of large magnification, feeling as if he is inside the patient’s body!
The robotic arms the surgeon navigates while sitting on a special console, offer stability, accuracy and flexibility of movements superior to any human hand.
As a result:
- tissue injury during surgery is avoided
- the risk of complications is dramatically reduced
- postoperative pain is minimized
- patients are mobilized immediately
- hospitalization is shorter
- recovery and return to daily activities is immediate