

Cancer of the Lower Esophagus – Gastroesophageal Junction
Cancer of the lower esophagus and gastroesophageal junction is a rapidly growing type of malignancy in the western population, whilst the incidence of most other cancers is declining.
This increasing trend in cases is attributed to the poor diet that characterizes the modern lifestyle, the sharp rise in obesity rates in the population and the consequent gastroesophageal reflux disease (GERD), which leads to Barrett’s esophagus and eventually to cancer.
Dr. Konstantinidis and his Surgical Team are pioneers internationally performing surgery assisted by the state-of-the-art robotic system Da Vinci Xi at Athens Medical Center, with impressive oncological outcomes and globally comparable low complication rates.
What is Lower Esophagus and Gastroesophageal Junction Cancer?
Cancer of the lower esophagus and gastroesophageal junction begins in the inner layer of the esophageal wall and grows outwards. It gradually spreads to the lymph nodes, as well as to the blood vessels in the chest and other nearby organs.
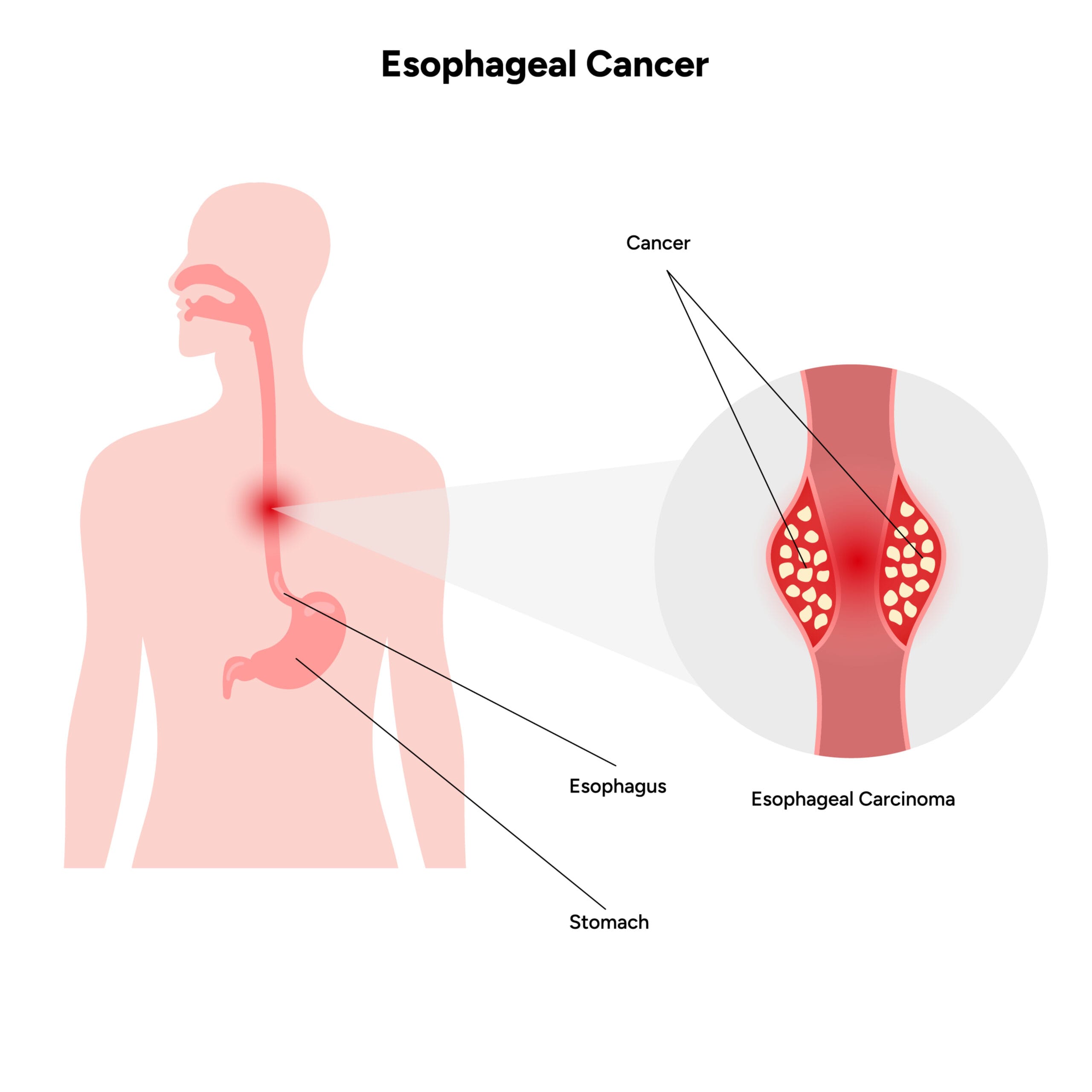
Cancer of the lower esophagus and gastroesophageal junction can also spread to the lungs, liver, stomach and other parts of the body.
The most common type of cancer in the lower esophagus and gastroesophageal junction is adenocarcinoma.
Why choose Dr. Konstantinidis?
Dr. K. M. Konstantinidis and his team possess vast experience in the field of laparoscopic and robotic surgery.
Dr. Konstantinidis is the pioneer of Robotic Surgery in Greece and one of the leading figures internationally in the field, having performed the largest series of General Surgery operations in Europe with the innovative Da Vinci® robotic system, including inguinal hernia surgeries.
What are the symptoms of Lower Esophageal Cancer and Gastroesophageal Junction?

At an early stage, cancer of the lower esophagus and gastroesophageal junction may be completely asymptomatic or may give mild symptoms that can also be due to a variety of causes, such as heartburn, atypical chest pain or indigestion.
Alternatively, patients may experience symptoms such as blood in the feces or anemia due to iron deficiency. Patients may report mild or intermittent dysphagia or a foreign body sensation.
These symptoms generally require diagnostic evaluation.
Some early cancers are diagnosed during endoscopic monitoring for Barrett’s esophagus.
Symptoms of lower esophageal cancer and gastroesophageal junction generally progress rapidly and become more pronounced as the tumor grows:
An initial difficulty in swallowing solids is followed by difficulty swallowing ground up food and finally liquids.
Weight loss and anorexia often occur in patients with more advanced disease. Odynophagia (painful swallowing) occurs in about half of patients.
Spreading of the cancer in the pericardium or mediastinum can cause posterior sternal pain or back pain, as well as abscess formation.
Hoarseness is usually associated with recurrent laryngeal nerve palsy (vocal fold paralysis).
Anemia and / or gastrointestinal bleeding and weakness may be present if the tumor is ulcerative.
What Causes Lower Esophageal and Gastroesophageal Junction Cancer?
Most cancers (adenocarcinomas) of the lower esophagus and gastroesophageal junction occur as a consequence of Barrett’s esophagus, a condition that results from chronic gastroesophageal reflux disease and subsequent esophagitis.
In Barrett’s esophagus, the wall (epithelium) of the lower esophagus is replaced by a wall similar to that of the stomach to protect it from refluxing gastric fluid as a result of chronic gastroesophageal reflux
Obesity is also associated with a significantly increased risk of esophageal cancer (adenocarcinoma), probably because obesity is a contributing factor to reflux.
According to studies, alcohol is not a significant risk factor, but smoking contributes to the development of the disease.
How is Lower Esophageal and Gastroesophageal Junction diagnosed?
The diagnostic evaluation of the patient with cancer of the lower esophagus and the gastroesophageal junction aims at the detection as well as the staging of the disease, in order to determine and immediately implement the appropriate treatment plan.
Barium meal with esophageal x-ray is an examination available in all health facilities with a radiology department, that should be performed on all patients with dysphagia, difficulty to swallow and other symptoms associated with lower esophageal and gastroesophageal junction cancer.
Upper gastrointestinal endoscopy to detect abnormal cells involves examining the esophageal wall, stomach, and the beginning of the small intestine with a flexible endoscope.
Endoscopy allows the doctor to view and take a sample of tissue (biopsy) from the mucosa of the upper gastrointestinal tract.
Biopsy endoscopy is the main method for diagnosing lower esophageal and gastroesophageal junction cancer.
Endoscopic ultrasound (EUS) is a useful tool for diagnosing lower esophageal and gastroesophageal junction cancer. Endoscopic ultrasound can detect small changes in the mucosa that are not clear on other types of diagnostic tests.
It also helps to determine the depth of the tumor in the esophageal wall and the involvement of the lymph nodes associated with the area.
Patients diagnosed with esophageal cancer also have a chest and abdomen CT scan to determine whether the cancer has spread.
How is the Cancer of the Lower Esophagus and Gastroesophageal Junction treated?
Decisions to treat lower esophageal and gastroesophageal junction cancer depend on the stage, size and location of the tumor, as well as the general health status of the patient.
Superficial, early, non-invasive cancers can be treated by endoscopic resection of the mucosa or endoscopic submucosal resection, if the superficial nature of the lesion has been confirmed by endoscopic ultrasound.
However, in most cases, treatment requires gastrectomy, that is, surgical removal of the entire tumor and surrounding tissues, all potentially malignant lymph nodes, and part of the stomach.
The gastrectomy can be performed with open surgery or with a minimally invasive method, i.e. laparoscopically and with robotic assistance.
Minimally invasive surgery is currently recommended by internationally recognized surgical teams as a means of improving postoperative outcomes in patients undergoing gastrectomy for lower esophageal and gastroesophageal junction cancer, especially when the disease is in its early stages.
Robotic gastrectomy maximizes the advantages of a minimally invasive approach, without the technical difficulties that accompany the traditional laparoscopic method or the heavy toll of open surgery.
The earlier the stage of cancer, the better the response to surgery, while preoperative chemotherapy and radiation provide additional benefits.
After treatment, patients are screened for recurrence by endoscopy and computed tomography of the neck, chest and abdomen at regular intervals of 6 months for 3 years and then annually.