

Hiatal Hernia – Gastroesophageal reflux
Gastroesophageal reflux disease (GERD) is a disorder in which stomach contents flow back into the esophagus causing various unpleasant symptoms.
Often, the disease occurs as a result of a hiatal hernia and as such it afflicts a large number of people who, thanks to the evolution of laparoscopic and robotic surgery and the development of new, minimally invasive surgical techniques, can now find immediate relief and regain a normal life.
Dr. Konstantinidis and his surgical team have extensive experience and know-how in repairing hiatal hernia and treating successfully gastroesophageal reflux.
Applying innovative robotic surgery techniques, Dr. Konstantinidis and his surgical team deal with over 100 cases of hiatal hernia annually, one of the largest series of patients in the world!
The techniques applied by Dr. Konstantinidis, like Nissen and Toupet fundoplication, are performed with the state of the art Da Vinci Xi HD robotic system, at Athens Medical Center, and have the highest success rates internationally and optimal postoperative course.

What is Gastroesophageal Reflux Disease?
In the lower part of the esophagus there is a small bundle of muscles in the shape ring, which is called the Lower Esophageal Sphincter (LES). The latter acts as a one-way valve, allowing only food to pass through and into the stomach. Normally, the lower esophageal sphincter closes immediately after the swallowing food to prevent the acidic fluids of the stomach from flowing back into the esophagus.
Gastroesophageal reflux occurs when the Lower Esophageal Sphincter does not work properly. As a result, the contents stomach, highly acidic, flow backwards and find a way out into the esophagus. The reflux of stomach acids into the lower part of the esophagus is harmful and dangerous, as if left untreated it can cause esophagitis, stenosis, ulcer, bleeding, dysplasia and even cancer.
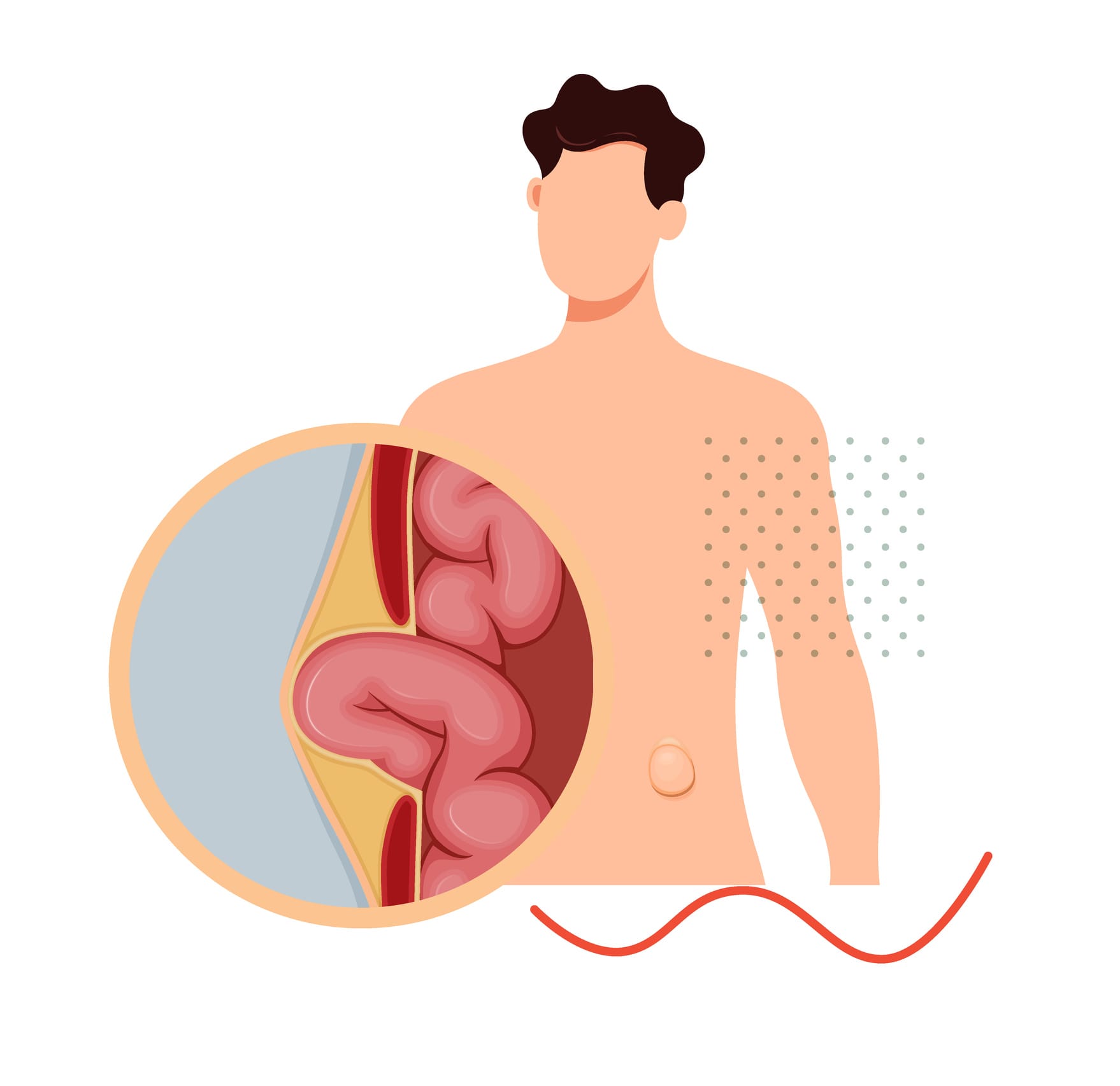
What is a Hiatal Hernia?
Hiatal hernia occurs when an anatomical structure of the abdomen, usually the stomach, is pushed into the thoracic cavity through a gap in the septum, which separates the abdomen from the thorax.
It is a fairly common condition and is estimated to affect about 10% of the population over the age of 40, a percentage that may progressively reach up to 50% in people over the age of 70.
Why choose Dr. Konstantinidis?
Dr. K. M. Konstantinidis and his team possess vast experience in the field of laparoscopic and robotic surgery.
Dr. Konstantinidis is the pioneer of Robotic Surgery in Greece and one of the leading figures internationally in the field, having performed the largest series of General Surgery operations in Europe with the innovative Da Vinci® robotic system, including inguinal hernia surgeries.
What are the symptoms of a Hiatal Hernia?

In its most common and mild form (Sliding – Type I) hiatal hernia is usually asymptomatic.
However, it can cause rash, heartburn, nausea or vomiting.
Paraesophageal hiatal hernias (Type II, III or IV) can cause more serious symptoms, such as:
Abdominal / chest pain
Abdominal bleeding
Voice change
Early satiety (after a small amount of food)
Occasional swallowing problem (especially solid food)
Shortness of breath or difficulty breathing after eating
The most common symptom of hiatal hernia, especially of the paraesophageal type, is gastroesophageal reflux.
What causes Hiatal Hernia?
The two main risk factors for hiatal hernia are age and too much weight: People over the age of 50 and those who are obese are at greater risk for developing this disorder.
Hiatal hernia is also caused by anything that increases intra-abdominal pressure, such as pregnancy, chronic cough, vomiting, chronic constipation, chronic obstructive pulmonary disease or even excessive weightlifting and intense physical pressure.
What types of Hiatal Hernia are there?
There are several types of hiatal hernia, which are categorized as follows:
Type I: Sliding hiatal hernia. This is the most common type of hiatal hernia, as it affects about 85% of the cases. Sliding hiatal hernia is a small hernia that usually does not require surgery.
Type II: Paraesophageal hiatal hernia. It accounts for about 5% of cases of hiatal hernia and it occurs when the upper part of the stomach pushes through an opening in the diaphragm and up into the chest.
Type III: Mixed hiatal hernia. It concerns a combination of the above two types and corresponds to a 10% of the cases.
Type IV: This category includes hiatal hernias that form when an anatomical structure other than the stomach passes into the chest through the septum.
The last three types, although much less common than the sliding hiatal hernia type, are potentially more dangerous, as they can cause severe symptoms.
How do I understand I have Gastroesophageal Reflux Disease?
Gastroesophageal reflux disease is characterized by symptoms and / or tissue damage resulting from repeated or prolonged exposure of the esophagus to stomach contents.
The symptoms of gastroesophageal reflux disease are often persistent, such as chronic heartburn, and vary from person to person. But sometimes there are no obvious symptoms and the presence of the disease is revealed when complications occur.
Recurrent heartburn is a symptom that many patients experience. Heartburn that occurs more often than once a week, becomes more severe or occurs at night and wakes the patient, can be a sign of a more serious condition and the advice of a doctor is recommended.
Chronic heartburn is the most common symptom of gastroesophageal reflux disease.
Other less common symptoms associated with gastroesophageal reflux disease include:
- Nausea – Vomiting
- Difficulty or pain when swallowing
- Dysphagia (the sensation of food sticking to the esophagus)
- Chronic sore throat
- Laryngitis
- Gingivitis
- Corrosion of tooth enamel
- Chronic irritation in the throat
- Acidic taste in the mouth
- Bad breath
Gastroesophageal reflux disease can cause chest pain that is often confused with the symptoms of a heart attack.
CAUTION! Never ignore your chest pain! In any case, seek immediate medical attention!
What are the complications of Gastroesophageal Reflux Disease?
If not treated in time and in its most severe forms, gastroesophageal reflux disease can cause a number of complications, such as:
- Esophagitis. Without treatment, esophagitis can cause bleeding, ulcers and chronic scarring of the esophagus.
- Barrett’s esophagus. In some cases of chronic disease, gastroesophageal reflux can cause a rarer form of esophagitis, which is associated with esophageal cancer.
- Esophageal stenosis
- Asthma and Respiratory Infections
How is Hiatal Hernia diagnosed?
There are various procedures and tests that may be required to diagnose hiatal hermia, depending on whether or not it is accompanied by gastroesophageal reflux disease, such as:
- Esophagoscopy
- 24-hour measurement of esophageal pH
- Chest X-ray
- Computed Tomography (CT)
- Endoscopy (Esophagogastroduodenoscopy – EGD)
- Esophageal manometry (examination with electrodes during which the pressure inside the esophagus is measured)
- Barium meal
- Transesophageal Echocardiography (TEE)
How Is Hiatal Hernia / Gastroesophageal Reflux Treated?
In its milder forms, gastroesophageal reflux disease can be treated conservatively with lifestyle changes, such as a healthier diet, more exercise, weight loss, smoking cessation, and reduced alcohol consumption.
Also, the treatment for gastroesophageal reflux disease may at an early stage include medication (proton-pump inhibitors), with the aim of lowering the pH of the stomach.
However, there are stages in the disease in which the administration of proton-pump inhibitors does not have the desired effect. This may result in the patient suffering and being exposed to the risk of possible complications in cases of long-term administration.
A review by the American Association of Gastroenterologists in 2017 lists dementia, kidney failure and digestive malignancies as some of the possible side effects of these drugs.
If conservative treatment does not bring results, as well as in more advanced stages of the disease, when it presents serious complications, such as Barrett’s esophagus, then surgery is preferred.
The goal of the surgery is to repair the hiatal hernia, which is the usual cause behind the manifestation of gastroesophageal reflux.
The surgery of choice for the treatment of hiatal hernia and subsequent gastroesophageal reflux disease is fundoplication, which is performed with laparoscopy internationally, to ensure excellent medical results by minimizing complications and ensuring optimal recovery of the patient.
Dr. Konstantinidis and his surgical team apply the most modern and minimally invasive techniques of fundoplication using the state-of-the-art Da Vinci Xi HD robotic system, at Athens Medical Center, with excellent success rates.
Hiatal hernia, GERD, Barret’s Esophagus Repair
ROBOTIC FUNDOPLICATION
What is Robotic Fundoplication?
An evolution of the equivalent laparoscopic technique, robotic fundoplication is the surgery of choice for the treatment of hiatal hernia involving the use a surgical robot to ensure maximum possible access to the problem area and precision in the surgeon’s movements.
With robotic fundoplication, the surgeon reshapes and corrects the hiatal hernia, strengthening the lower esophageal sphincter valve. This is achieved by wrapping the upper stomach (fundus) and around the lower part of the esophagus.
There are different techniques of fundoplication depending on the degree of winding of the stomach fundus around the esophagus:
- Nissen fundoplication or 360 ° fundoplication
- Toupet fundoplication or 270 ° fundoplication
- Dor fundoplication or 180% fundoplication
Having performed hundreds of robotic surgical procedures including fundoplication for the repair of hiatal hernia since 2006, Dr. Konstantinidis is an international pioneer in the robotic repair of the hiatal hernia, performing surgeries of high precision and optimal medical outcome with the assistance of the most modern surgical robot in the world, the Da Vinci Xi HD, at Athens Medical Center.
What type of surgery should I choose?
The condition of the esophagus, as revealed by the thorough preoperative evaluation that all patients undergo, largely determines the type of surgery that will be chosen for the repair of a hiatal hernia.
If the preoperative evaluation shows that the esophagus is functional, the preferred procedure is Nissen fundoplication, which significantly strengthens the valve of the lower esophageal sphincter.
This is also the most common surgery for treating gastroesophageal reflux.
However, if it is determined that the patient’s esophagus is not functional and does not perform proper peristalsis (i.e., the wave-like contractions that allow food to move towards the stomach), then a partial fundoplication technique such as the Toupet or Dor procedure is selected.
In this way, the proper functioning of the esophagus is ensured postoperatively.
How is Robotic Fundoplication carried out?
With the assistance of the robotic system, the surgeon makes 4-5 small incisions in the skin (5 mm long each), without cross-cutting the muscle. The laparoscope and other laparoscopic instruments customized for use from the robotic arm are inserted through these incisions.
The laparoscope, which is connected to a tiny, state-of-the-art video camera, allows the surgeon to see the patient’s internal organs at a magnification of 10-15 times on a screen.
What are the advantages of Robotic Fundoplication?
Robotic fundoplication incorporates all the advantages of laparoscopic fundoplication and takes them to the next level.
In particular, the advanced features of the Da Vinci Surgical Robot System Xi Version robotic platform, such as 3D imaging, improved ergonomics compared to its predecessors, the more advanced and flexible tools, combined with a surgeon’s many years of experience in laparoscopic and robotic surgery, are maximized and the outcome is impressive:
- Postoperative pain is minimal, thanks to the absence of incisions.
- The majority of patients return home the next day with minimal use of painkillers.
- The cosmetic result is excellent.
- Recovery is immediate and return to daily activities very short
In addition, the planning of the operation by Dr. Konstantinidis and his surgical team as well as the default positions of the incisions are pioneering at a global level and have excellent results.
The most important advantage, however, is the maximum possible avoidance of complications. The incomparable precision and ease of movement offered by the robotic system ensures that tissues or other organs will not be injured during the operation.
In particular, the risk of injury to the spleen (and therefore splenectomy), liver and esophagus is avoided, the pneumogastric nerve and its branches are preserved and the nerves of the area are generally protected and maintained in their normal positions.
Robotic fundoplication achieves excellent results in the cases of very heavy, type III or IV hiatal hernias, which in other types of surgery may even require open thoracotomy!
Similarly, robotic fundoplication ensures excellent results in obese patients or with anatomical variants.
LAPAROSCOPIC FUNDOPLICATION
What is Laparoscopic Fundoplication?
Laparoscopic fundoplication is the surgery of choice for the repair of hiatal hernia and the treatment of gastroesophageal reflux disease.
During laparoscopic fundoplication, the surgeon wraps the upper part (fundus) of the stomach around the lower esophageal sphincter, reinforcing its valve and thus preventing the reflux of the contents of the stomach and repairing the hiatal hernia.
There are two techniques used:
- Nissen laparoscopic fundoplication or 360 ° fundoplication and
- Toupet laparoscopic fundoplication or 270 ° fundoplication
Laparoscopic fundoplication is a procedure that lasts 3 to 4 hours. To perform it, 4-5 small incisions (about half a centimeter each) are made in the skin, without cutting muscles, through which the surgeon passes the laparoscope (carrying a state-of-the-art microcamera) and the other surgical instruments.
How Safe is Laparoscopic Fundoplication?
Laparoscopic fundoplication is considered a safe surgical procedure with minimal risk of complications.
However, it requires precision and skill in manipulations and its success is directly related to the experience of the surgeon, as well as his knowledge of the anatomy of the area.