

Esophageal achalasia
Esophageal achalasia is a rare but serious disorder that is accompanied by unpleasant symptoms, such as difficulty to swallow, and if neglected carries health risks.
Achalasia is considered a precancerous condition, because after about 15 – 25 years esophageal cancer develops in 1% – 10% of patients.
Thanks to contemporary methods of robotic / laparoscopic surgery, the treatment of esophageal achalasia is safer and more immediate than ever, without the hassle of open surgery and with lasting medical outcomes!

What is esophageal achalasia?
Achalasia is a rare disorder of the esophagus, the tubular organ through which food travels from the throat to the stomach.
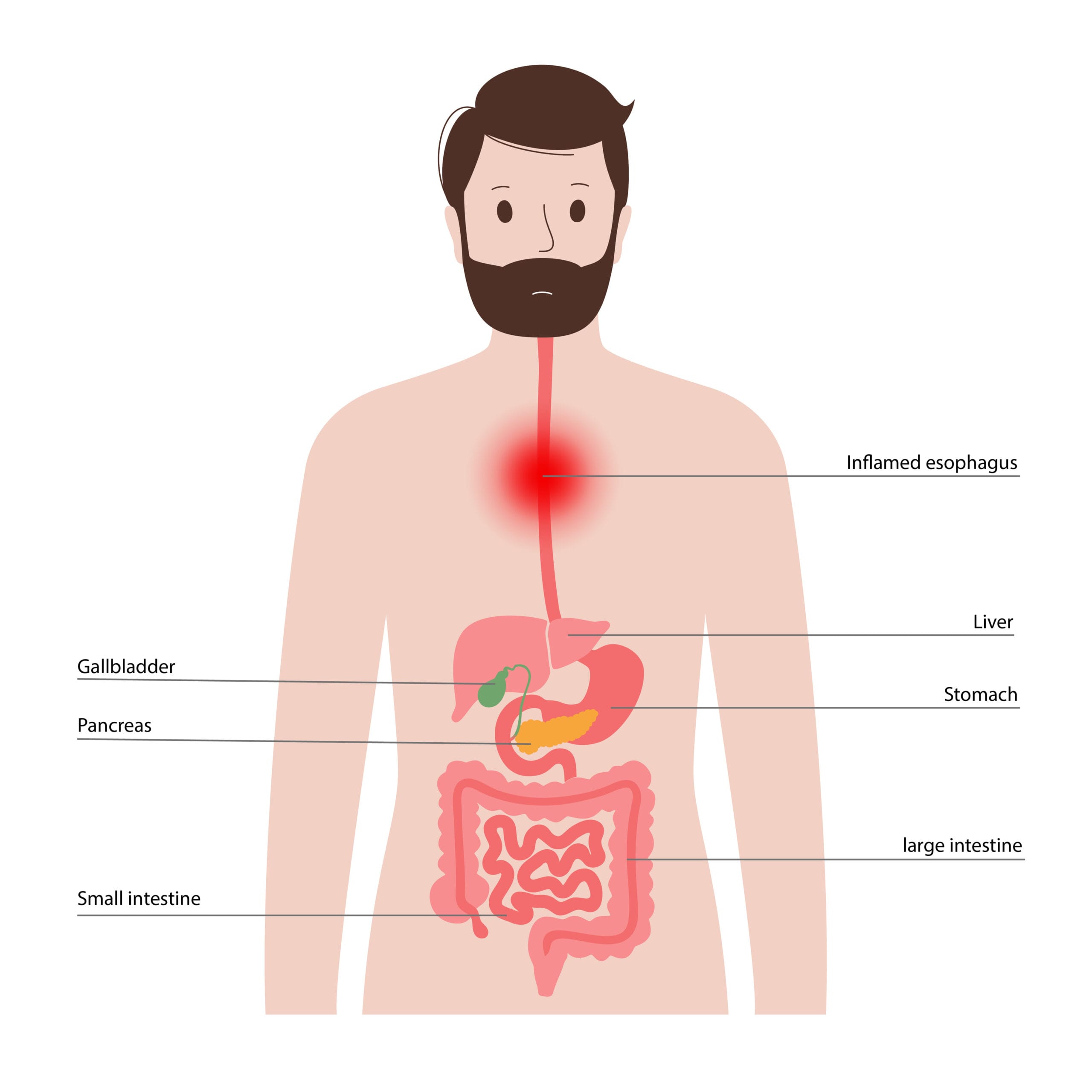
In achalasia, the esophagus is unable to complete its peristaltic movements and the Lower Esophageal Sphincter does not open sufficiently for food to pass through, because it is in a state of constant spasm.
As a result, food is not properly pushed into the stomach and instead remains in the esophagus for a long time.
Why choose Dr. Konstantinidis?
Dr. K. M. Konstantinidis and his team possess vast experience in the field of laparoscopic and robotic surgery.
Dr. Konstantinidis is the pioneer of Robotic Surgery in Greece and one of the leading figures internationally in the field, having performed the largest series of General Surgery operations in Europe with the innovative Da Vinci® robotic system, including inguinal hernia surgeries.
What are the symptoms of esophageal achalasia?

The symptoms of achalasia usually appear gradually and include the following:
Dysphagia. It is the most usual symptom of esophageal achalasia, as patients have difficulty swallowing.
Regurgitating food or saliva. Because food cannot be pushed into the stomach it is accumulated in the esophagus, at times coming out in the form of vomit.
Respiratory infections. Regurgitating food during sleep can cause coughing overnight and in the long run contributes to the development of pneumonia and pulmonary abscesses.
Esophagitis and esophageal ulcers. In achalasia, food stays and is decomposed in the esophagus, a condition that causes chronic inflammation.
Weight loss. Poor nutrition, as a result of the improper pushing of food from the esophagus into the stomach, causes weight loss.
How is esophageal achalasia diagnosed?
Diagnosis is the first step in treating the condition. The symptoms are mild at first or may point to other conditions.
Gastroscopy is the first screening test that primarily rules out other conditions with similar symptoms, such as esophageal cancer.
Then, because achalasia essentially belongs to the motor disorders of the esophagus, a dynamic assessment of the esophagus is necessary.
Esophageal barium swallow and meal X-ray is an examination available in all health facilities with a radiology department, that should be performed on all patients with dysphagia and may make the initial diagnosis of achalasia or other esophageal motility disorders.
The diagnosis is substantiated by esophageal manometry, a test that measures pressures along the entire length of the esophagus and also gives an idea of the overall peristalsis of the esophagus.
In recent years, High Resolution Manometry (HRM) has been widely used, as it easily, quickly, and accurately delivers all the aforementioned parameters.
With this examination the staging and classification of the disease is achieved.
The treatment is individualized and factors, such as the length of the required myotomy, are adjusted to each patient according to the imaging findings in order to achieve the optimal functional result.
How is esophageal achalasia treated?
Conservative treatment, with the administration of special medication aimed at relaxing the Lower Esophageal Sphincter, offers only temporary relief to the condition.
The same goes for endoscopic interventions, such as dilations, which aim to widen the diameter of the Lower Esophageal Sphincter. The duration of relief from symptoms after dilation is usually unsatisfactory.
Lastly, botox injection is used to paralyze the sphincter and improve swallowing. But here too the relief is temporary.
The most definitive treatment of esophageal achalasia is surgery (myotomy) laparoscopic or robotic, for optimal medical results.
Open myotomy procedures have now been abandoned.
Esophageal achalasia - HELLER myotomy with Dor vaulting
Laparoscopic Myotomy
What is Laparoscopic Myotomy?
The operation of choice for the treatment of esophageal achalasia involves the so-called laparoscopic myotomy according to Heller and in some cases is accompanied by laparoscopic fundoplication according to Dor or Toupet to prevent reflux from the stomach into the esophagus.
In this operation, the surgeon opens small holes of a few millimeters in the patient’s abdomen, through which special laparoscopic tools are inserted, and then makes a small incision in the muscular lining of the esophagus, about 6 cm long.
The purpose is to cross the muscle fibers of the lower esophageal sphincter, in order to relax its pathological and prolonged contraction and to restore the normal pushing of the food into the stomach.
Robotic Myotomy
What is a Robotic Myotomy?
Robotic myotomy is an evolution of the laparoscopic operation, with the assistance of a robotic system. The use of the robot offers the surgeon unparalleled accuracy and ease of movement, as well as impressive visibility, thanks to the ability to magnify the surgical field on a screen.
During robotic myotomy, special surgical instruments are inserted through holes about 5 millimeters in size, opened in the patient’s abdomen.
The surgeon then makes a few centimeters long myotomy on the muscular lining of the esophagus. If necessary, the operation is accompanied by a Dor or Toupet fundoplication of the stomach around the lower esophagus, in order to avoid postoperative fluid reflux.
Robotic myotomy takes about 1 to 2 hours.
How Safe is a Robotic Myotomy?
The advantages of the robotic system are crucial for the success of the surgery, as myotomy is an operation that requires great precision from the surgeon when performing the incision in the esophageal and stomach tissue.
The use of the robot ensures the maximum possible accuracy in the length and depth of the myotomy, as well as in carrying out the fundoplication.
Thus, the surgeon avoids the risk of complications that sometimes occur with other types of myotomy procedures, such as bleeding or injury to the spleen and other viscera, which could result in a splenectomy or other procedure to remove the injured organ.
What happens after surgery?
The patient stays in the hospital for a day or two, depending on how soon he/she will be fed properly.
Before the patient is first fed after surgery, the passing of the food from the esophagus into the stomach is examined, a radiological test in which fluid is taken from the patient to confirm the normal functioning of the esophagus.
After the patient is fed, he/she is discharged and soon returns to his/her daily habits free from the torturous symptoms of the disorder.