

Thyroid Cancer
Thyroid cancer is a relatively rare form of malignancy, which has a good prognosis if the patient is diagnosed early and treated appropriately.
Surgery is the main treatment for thyroid cancer and it involves the removal of the cancer-infected organ with a procedure called thyroidectomy.
In recent years, thyroidectomy is performed with minimally invasive techniques and especially with the use of surgical robots.
While ensuring optimal oncological results, robotic surgery minimizes complications from surgery and offers the best cosmetic result, with no visible scar (one of the disadvantages of conventional thyroidectomy, especially in young women).
Dr. Konstantinidis and his Surgical Team have extensive experience and specialization in the treatment of thyroid cancer, having performed a great number of thyroidectomies.
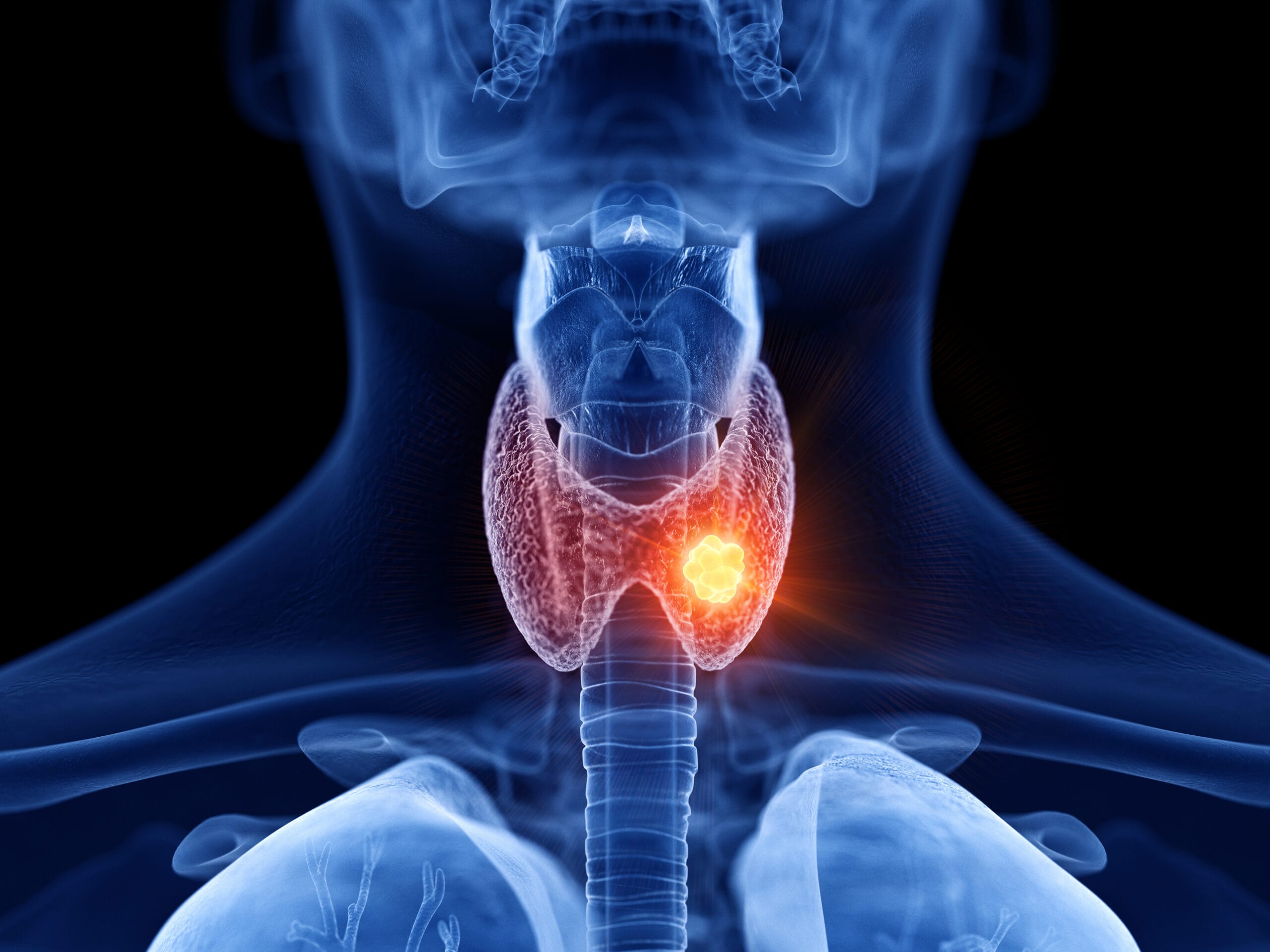
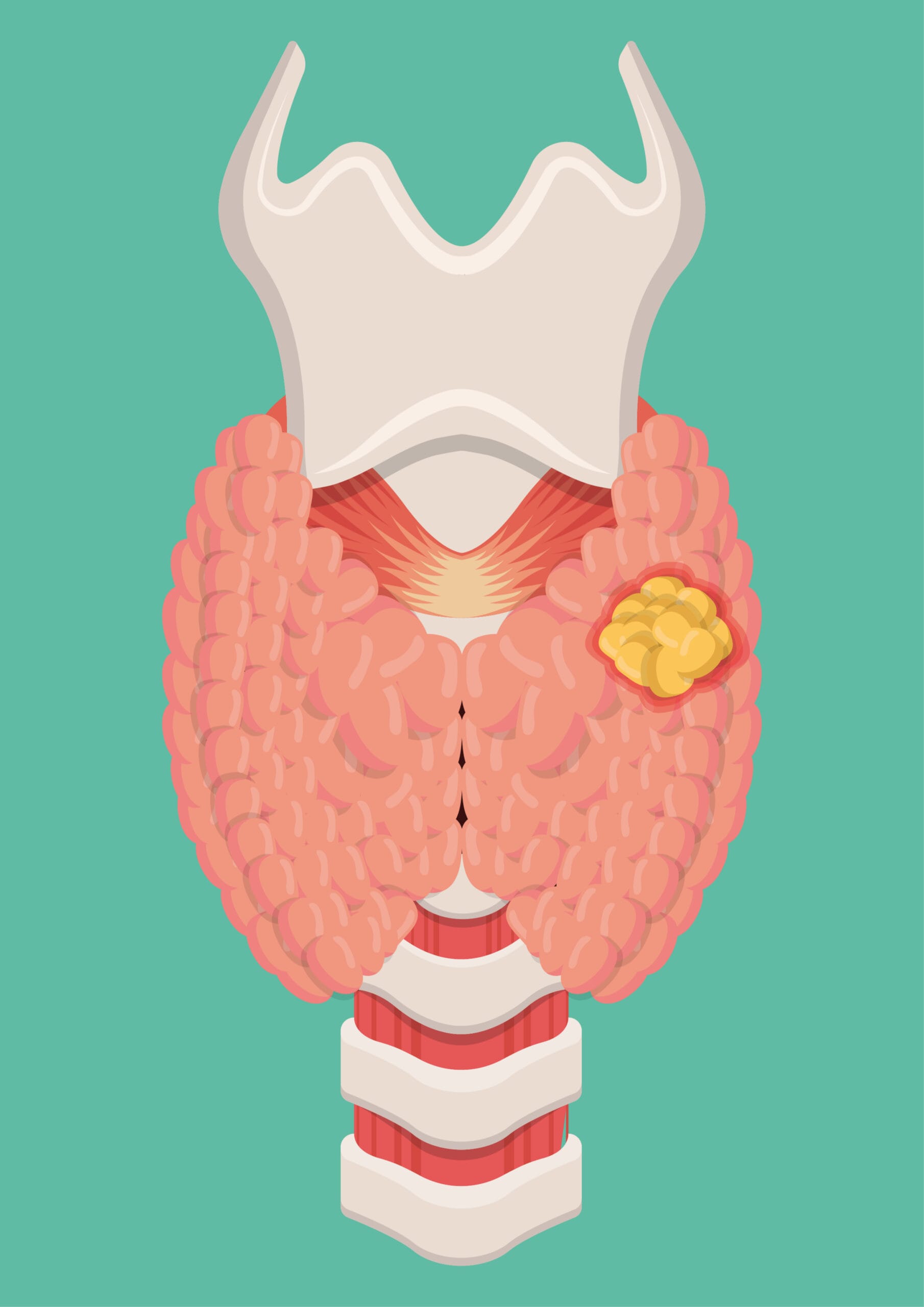
What is the Thyroid Gland?
The thyroid gland is one of the most important glands in the human body.
Its purpose it to manage the most important functions of the body, regulating metabolism and growth and indirectly our mental health and balance.
The thyroid gland produces and stores several vital hormones (triiodothyronine T3, thyroxine T4) which are then channeled through the bloodstream to the rest of the body.
What is Thyroid Cancer?
Thyroid cancer is a relatively rare form of malignancy (less than 1% of all cancers). However, it is the most common endocrine cancer.
Thyroid cancer usually has a good prognosis and is categorized into:
- Carcinomas that originate from follicular cells and are the most common (papillary and follicular carcinomas)
- Myeloid carcinoma, which originates from parathyroid cells and is the least common
In most cases, thyroid cancer is discovered accidentally, in the form of a solitary nodule (local swelling) after a clinical examination or after observation of the patient himself or a person in his environment.
Sometimes the diagnosis is made postoperatively, after the removal of the gland for the purpose of treating goiter.

Do you want to know more about Thyroid Cancer ;
Why choose Dr. Konstantinidis?
Dr. K. M. Konstantinidis and his team possess vast experience in the field of laparoscopic and robotic surgery.
Dr. Konstantinidis is the pioneer of Robotic Surgery in Greece and one of the leading figures internationally in the field, having performed the largest series of General Surgery operations in Europe with the innovative Da Vinci® robotic system, including inguinal hernia surgeries.
What are the symptoms of Thyroid Cancer?

Thyroid cancer usually develops slowly, without many obvious signs or symptoms. However, some people may experience one or more of the following symptoms:
A lump in front of the neck
hoarseness
swollen glands in the throat
difficulty swallowing
difficulty breathing
pain in the throat or neck
persistent cough not caused by a cold
Although a painless lump in the neck is the most common sign, thyroid nodules are common and benign in 90% of adults.
Underactive or overactive thyroid gland (hypothyroidism or hyperthyroidism) is not a symptom of thyroid cancer.
What are the risk factors for Thyroid Cancer?
The exact cause of thyroid cancer is unknown, but some factors have been found to increase the risk of developing it:
Exposure to radiation. A small number of cases of thyroid cancer are due to radiation therapy in the head and neck area in childhood or to living in an area with high levels of radiation in the environment. Thyroid cancer usually takes 10-20 years to develop after radiation exposure.
Heredity. Only about 5% of thyroid cancers are hereditary. Having a first-degree relative (parent, child or sibling) with thyroid cancer may increase the risk. Some hereditary genetic conditions, such as familial adenomatous polyposis or Cowden syndrome, may also increase the risk of thyroid cancer.
Obesity. Being overweight or obese can also increase your risk of developing thyroid cancer.
Thyroid disorders. Conditions of the thyroid gland, such as thyroid nodules, multinodular goiter or inflammation of the thyroid gland (thyroiditis), slightly increase the chance of developing thyroid cancer.
How is Thyroid Cancer diagnosed?
Thyroid cancer is often diagnosed with a standard throat examination during a general physical examination. They can also be detected randomly on imaging tests (ultrasound, CT scan) that may have been performed for other reasons.
In particular, the diagnosis of thyroid cancer may include a combination of the following tests:
- Physical examination: The doctor feels the cervix, thyroid gland and lymph nodes, for unusual growths or swelling. Occasionally, the larynx may be examined simultaneously with a laryngoscope.
- Blood tests: There are several types of blood tests that can be done to diagnose thyroid cancer, such as thyroid hormone levels, triiodothyronine (T3) and thyroxine (T4), thyroid stimulating hormone (TSH) and thyroglobulin antibodies (TgAb), as well as cancer marker tests such as calcitonin and carcinoembryonic antigen (CEA) levels.
- Ultrasound
- Biopsy: The most effective preoperative method for the differential diagnosis of benign and malignant thyroid nodules is the cytologic examination of tissue obtained with a fine needle aspiration (FNA). If the FNA biopsy does not show clear results, a surgical biopsy may be performed, in which the nodule and possibly the affected thyroid gland is removed.
- Elastography, to evaluate the hardness of a nodule.
- Thyroid scintigraphy, for the visual display of functional thyroid tissue.
- Whole body scintigraphy with Iodine 131, for the detection of local recurrence and metastases of thyroid cancer.
- X-ray, to detect possible metastases, e.g. in the lungs
- Computed tomography (CT), for accurate measurement of the tumor, especially in anatomical points that are not visible on ultrasound, as well as the detection of possible metastases.
- Positron emission tomography (PET) or PET-CT: PET scan is usually combined with computed tomography (PET-CT).
How Is Thyroid Cancer Treated?
The treatment is mainly surgical for all types of thyroid malignancy and it involves the removal of the gland (total thyroidectomy), as well as in some cases the removal of the lymph nodes, if the disease has been found or suspected to have spread.
Most patients undergo thyroidectomy initially, and all receive hormone therapy postoperatively.
Usually, depending on the type of thyroid cancer and in collaboration with the Nuclear Medicine team, patients are provided with a therapeutic dose of radioactive iodine to destroy any remaining malignant cells in the area.
Rarely, the patient may undergo radiotherapy preoperatively or in the form adjunctive therapy in anaplastic carcinomas, while even more rarely, chemotherapy is recommended.
The exact treatment plan is determined by the oncology board, i.e. an interdisciplinary team of specialists, such as endocrinologist, oncologist, radiologist and general surgeon specializing in endocrine gland surgery.
Thyroidectomy Using a Nerve Stimulator
How is the thyroid gland surgically removed?
Thyroid surgery is a demanding surgery, which must be performed by a specialized surgeon.
The gland is located in a sensitive area adjacent to many vital organs and formations (nerves, vessels, trachea, esophagus).
The prevailing view is that the entire gland should be removed (total thyroidectomy), except in rare cases where part of the gland is removed (partial thyroidectomy).
During thyroidectomy, a small incision of 3-4 cm is made in the cervix.
The advanced techniques of microsurgery allow surgeons to remove the entire thyroid gland, without cutting the muscles, having the surgical field enlarged (so they recognize and protect all the surrounding sensitive structures).
In addition, the preservation and preservation of the lower laryngeal nerves is achieved by using a specialized electronic machine (neurostimulator).
During the operation, instead of the conventional tools, specialized ultrasound devices, Laser and R-F (radio frequencies) are used helping to render the operation bloodless and without injuries.
The operation is completed with plastic surgery and without the need for drainage.
The patient is discharged the next day.
In conclusion, fine knowledge of the anatomy of the cervix and its variants, combined with surgical experience and modern technological equipment in the operating room, provide the guarantees for a perfect and above all safe surgery.
Robotic Thyroidectomy
What is Robotic Thyroidectomy?
With the advancement of medical and surgical technology, there has been a tremendous development in surgical approaches to thyroidectomy.
Robotic thyroidectomy has become increasingly popular worldwide, attracting both surgeons and patients seeking new and innovative techniques for removing cancer from the thyroid gland and surrounding area with superior cosmetic results compared to conventional open surgery.
Robotic thyroidectomy eliminates the neck scar, as it allows access to the thyroid gland through an incision under the arm. This is called the axillary approach.
This incision is 5-7 cm long but is hidden – not in front and in the center, like the scars on the neck from open or even most endoscopic thyroidectomies.
The selection of patients for robotic thyroidectomy is made with strict criteria that have to do mainly with their body type.
Robotic thyroidectomy is performed using the da Vinci Xi robotic system, with great success. This system has:
Four robotic arms, which operate like human hands, but with greater capabilities and better performance. They can catch things, twist and turn – and they are incredibly small. Robotic arms offer unparalleled precision, stability and flexibility of movements.
3D camera: A high-definition camera offers a 3D image of the thyroid. Surgeons can digitally zoom in and get an even more detailed view of the surgical field, as if they were inside the patient’s body.
Console: The surgeon sits on a console, through which he navigates the robotic arms based on the 3D image of the surgical field that the camera sends to the console screen.
The robotic arms and the 3D camera are inserted in the area to be operated through the incisions. The surgeon can then precisely remove part or the entire thyroid, depending on what the patient needs.
What are the advantages of Robotic Thyroidectomy?
Robotic thyroidectomy combines all the advantages of conventional laparoscopic surgery as a minimally invasive method, such as minimizing complications, postoperative pain and hospitalization, as well as recovery time, with the unique capabilities offered by robotic technology:
- no scar on the neck
- better view of the surgical field, which allows better accuracy and attention to the surrounding healthy tissue during thyroid resection
- improved recognition of critical structures, such as the laryngeal nerve and parathyroid glands, thanks to digital zoom and 3D imaging
- enhanced dexterity in certain areas: Robotic instruments give the surgeon freedom of movement in 360 degrees allowing for better and easier handling of certain parts of the thyroid
What are the complications of Thyroidectomy?
The use of the nerve stimulator in combination with the large magnification of the surgical field offered by the special glasses of the surgical team have eliminated the serious complications.
Potential complications of surgery are hypocalcaemia (usually transient), which is why we often give calcium for a short time. Transient hoarseness is also rare.
The likelihood of permanent damage depends on the severity of the problem and the experience of the surgical team. With the use of a nerve stimulator, the laryngeal nerves are more easily identified and protected, eliminating the risk of damage.
To prevent hypothyroidism, the patient receives thyroid hormone for life.